Autoimmune hepatitis is a disease in which the immune system, the body’s defenses, mistakenly attacks the liver itself and causes inflammation. Without treatment it can damage the liver progressively and lead to cirrhosis, but the good news is that, diagnosed early and treated appropriately, it has an excellent prognosis.
It is more common in women and can appear at any age. It can present in two very different ways: as an acute hepatitis, sometimes severe, or as a chronic disease that advances silently over years. That is why it is worth knowing about and investigating when liver enzymes are elevated without a clear cause.
What is autoimmune hepatitis?
Hepatitis means inflammation of the liver. There are many reasons the liver can become inflamed: infections by hepatitis viruses, fat buildup, certain medications or iron overload, among others. In one group of diseases, the problem lies in the immune system itself, which stops recognizing the body’s tissues as its own and attacks them.
Autoimmune diseases of the liver include:
- Autoimmune hepatitis.
- Primary biliary cholangitis, formerly called primary biliary cirrhosis.
- Primary sclerosing cholangitis.
- Overlap syndromes, in which features of more than one of these diseases are combined.
This article focuses specifically on autoimmune hepatitis.
Causes
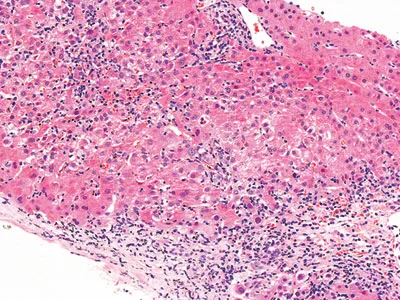
Liver inflammation seen under the microscope in a person with autoimmune hepatitis
It is not known exactly why autoimmune hepatitis develops. There is a genetic predisposition, as with other autoimmune diseases, and sometimes an environmental factor triggers the process in a susceptible person. Occasionally an infectious trigger is identified, such as the hepatitis A virus, which can start the inflammation and keep it going even after the infection has cleared. Some medications, such as nitrofurantoin and minocycline, can also trigger a hepatitis with autoimmune features.
Clinical features
Autoimmune hepatitis mainly affects women, although it can occur in men and at any age. Its course fluctuates and symptoms vary. It is not unusual for it to be diagnosed through laboratory findings in people who feel well.
When symptoms are present, they tend to be nonspecific: fatigue, nausea, abdominal pain and joint aches. The way it presents can vary widely:
- Acute presentation: some patients present as an acute hepatitis, with marked jaundice. In rare cases it progresses to acute liver failure, with a drop in prothrombin time and encephalopathy.
- Chronic presentation: in many patients the disease advances slowly and is detected through elevated liver enzymes or once there are already signs of cirrhosis, such as ascites, dark urine or bleeding from varices.
Some people also have other associated autoimmune diseases, such as thyroiditis, autoimmune hemolytic anemia, immune thrombocytopenic purpura, type 1 diabetes or celiac disease.
Autoimmune hepatitis is classified into two types:
- Type 1: the most common form. It can occur at any age and is usually associated with antinuclear antibodies (ANA) or anti-smooth muscle antibodies (ASMA).
- Type 2: more typical of children and adolescents. Its characteristic marker is anti-liver-kidney microsomal antibodies (anti-LKM1).
Diagnosis
No single test confirms the disease. The diagnosis is based on combining clinical, laboratory, antibody and biopsy findings, and on ruling out other causes.
Blood tests show:
- Elevated liver enzymes (AST and ALT), with normal or only slightly altered alkaline phosphatase and GGT. In more advanced cases there may also be a rise in bilirubin, a drop in albumin and prolongation of the prothrombin time.
- Elevated immunoglobulin G (IgG), a very characteristic finding.
- Autoantibodies. Most patients have at least one. The most useful are antinuclear antibodies (ANA), anti-smooth muscle antibodies (ASMA) and anti-LKM1. In some cases others are sought, such as anti-soluble liver antigen (anti-SLA).
The liver biopsy is a central part of the diagnosis. The typical findings are interface hepatitis and inflammation with abundant plasma cells.
Before confirming the diagnosis it is essential to rule out other causes of liver damage: viral hepatitis, excessive alcohol use and hepatotoxic medications. Diagnostic criteria exist that combine all these elements into a score and allow the disease to be classified as probable or definite. The response to treatment also helps confirm the diagnosis.
Treatment
The goal of treatment is to switch off the inflammation and bring the disease into remission, meaning normal liver enzymes and IgG, kept that way over time. Not everyone needs treatment right away, but most patients benefit, especially those with very high liver enzymes, elevated IgG or significant inflammation on biopsy. In children it is almost always started at diagnosis.
Treatment relies on medications that dampen the immune system and is organized in two phases:
- Inducing remission. Corticosteroids are used, usually prednisone, which control the inflammation quickly. In many cases they are combined from the start or early on with azathioprine, which allows the corticosteroid dose to be reduced sooner and limits its side effects.
- Maintenance. Once remission is reached, prednisone is tapered to the lowest necessary dose and azathioprine is continued. Treatment is usually long, lasting several years, and in many patients it is continued indefinitely because of the risk of relapse if it is stopped.
Budesonide is a corticosteroid that acts mainly in the liver and has fewer body-wide effects. In a randomized trial, combined with azathioprine, it induced remission with fewer side effects than prednisone in patients without cirrhosis, so it is an option in selected cases. It is not recommended once cirrhosis is present. For those who do not respond to or cannot tolerate standard treatment, other immunosuppressants such as mycophenolate or tacrolimus are used, always prescribed by a specialist.
These medications can have side effects. Corticosteroids favor weight gain, osteoporosis, diabetes and high blood pressure; azathioprine can lower white blood cells and, less often, cause pancreatitis or liver damage. For this reason treatment requires regular monitoring of blood tests and should be supervised by a hepatologist with experience.
Prognosis
The prognosis of autoimmune hepatitis is good when it is treated early. Without treatment it can progress toward cirrhosis, but with the right therapy most patients reach remission and avoid advanced damage. Even in those who present with cirrhosis, controlling the inflammation can reduce fibrosis over the years.
In cases that reach decompensated cirrhosis or that present as acute liver failure, liver transplantation is a very good option, with excellent survival. The disease can recur in the transplanted liver in some patients, but it is usually controlled by adjusting the immunosuppression.
See also
References
- Mack CL, et al. Diagnosis and Management of Autoimmune Hepatitis in Adults and Children: 2019 Practice Guidance and Guidelines From the AASLD. Hepatology. 2020;72(2):671-722.
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines on the management of autoimmune hepatitis. J Hepatol. 2025;83(2):453-501.
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Autoimmune hepatitis. J Hepatol. 2015;63(4):971-1004.
- Manns MP, et al. Budesonide induces remission more effectively than prednisone in a controlled trial of patients with autoimmune hepatitis. Gastroenterology. 2010;139(4):1198-1206.
Related articles
Primary biliary cholangitis (formerly primary biliary cirrhosis)
Primary biliary cholangitis (formerly primary biliary cirrhosis) is an autoimmune disease of the bile ducts. What it is, how it is diagnosed and how it is treated.
Primary sclerosing cholangitis (PSC)
Primary sclerosing cholangitis inflames and narrows the bile ducts, is linked to ulcerative colitis and is diagnosed with MR cholangiography. What it is and how it is managed.
Bilirubin: what it is and what a high level means
High bilirubin can be due to hemolysis, Gilbert syndrome, bile duct obstruction or liver disease. How to interpret this test based on its pattern.