On this page
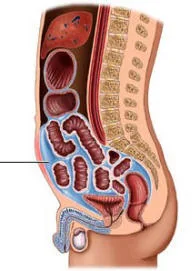
Ascites is the buildup of fluid in the abdominal cavity. Although it has many possible causes, from infections to heart failure or cancer, by far the most common is cirrhosis. In a person with liver disease, the appearance of ascites marks the shift to what is called decompensated cirrhosis and is often the first visible sign that the liver is no longer coping well.
This article focuses on ascites of liver origin: why it happens, how it is evaluated, how it is treated, and why it matters to recognize its complications early, especially infection of the fluid.
Why does ascites happen in cirrhosis?
In cirrhosis, scar tissue blocks the flow of blood through the liver. This raises the pressure in the portal vein, the vein that carries blood from the intestine to the liver, a phenomenon called portal hypertension. That high pressure, together with circulatory changes that make the kidney retain salt and water, causes fluid to leak out of the vessels and collect in the abdomen. This is why ascites almost always appears once cirrhosis is already advanced.
Symptoms of ascites
Ascites usually builds up gradually. Many people first notice weight gain from fluid retention before they see the abdomen enlarge. The most common symptoms are:
- Increased waist size, with a sense of bloating or heaviness.
- Weight gain over a few days or weeks.
- Leg swelling (edema), which usually accompanies ascites.
- Early fullness, that is, feeling full after eating little.
- Shortness of breath when the fluid is large and pushes on the diaphragm.
Anyone with liver disease who notices these changes should seek care. The onset of ascites always calls for a medical evaluation.
How is ascites evaluated?
The workup has two goals: to confirm that the fluid is due to portal hypertension and to rule out complications. The evaluation includes:
- Abdominal ultrasound, which confirms the fluid and assesses the liver. A Doppler study of the portal vein is often added to check that it is open.
- Blood tests, such as kidney function, electrolytes and albumin.
- Diagnostic paracentesis. This means removing a small sample of fluid with a fine needle to analyze it. It is a safe and essential procedure: it is recommended in everyone presenting with ascites for the first time or admitted to hospital.
A key test on the fluid is the serum-ascites albumin gradient (SAAG), calculated by subtracting the albumin in the ascitic fluid from the albumin in the blood. A SAAG of 1.1 g/dL or higher reliably indicates that the ascites is due to portal hypertension, as in cirrhosis. The same sample is used to count white blood cells, especially neutrophils, to rule out infection.
Treatment of ascites

Treatment aims to remove the excess salt and water, and is adjusted to the amount of fluid and each person’s response.
- Salt restriction. This is one of the most important measures. A low-sodium diet is recommended, avoiding cured meats, chips, canned goods, concentrated broths and packaged food. Fluid intake, in contrast, does not need to be restricted unless the sodium in the blood drops significantly.
- Diuretics. These are the foundation of drug treatment. The main one is spironolactone, to which furosemide is often added to increase and balance its effect. They require monitoring of kidney function and electrolytes, because too high a dose can harm the kidney.
- Large-volume paracentesis. When the ascites is very large or does not respond to diuretics, the fluid is drained with a needle through the abdomen, sometimes several liters. If more than 5 liters are removed, intravenous albumin is given to prevent circulatory and kidney problems.
- TIPS. In cases where ascites keeps returning despite treatment (refractory ascites), a stent can be placed connecting the portal vein to a vein in the liver, lowering the portal pressure. It is inserted through a catheter via a vein in the neck. One of its risks is triggering hepatic encephalopathy.
Bed rest, once advised, is no longer considered a central part of treatment.
Spontaneous bacterial peritonitis: a serious complication
Spontaneous bacterial peritonitis (SBP) is infection of the ascitic fluid without an obvious cause, such as a bowel perforation. It is one of the most dangerous complications of ascites and can be life-threatening.
It should be suspected, and prompt care sought, in the presence of warning signs such as:
- Fever or chills.
- Abdominal pain or increased tenderness of the abdomen.
- Worsening general condition, confusion or drowsiness (which may reflect encephalopathy).
- Worsening kidney function or of the response to diuretics.
The diagnosis is made with a paracentesis: SBP is confirmed when the fluid has 250 or more neutrophils per cubic millimeter. Treatment must begin immediately with intravenous antibiotics, usually a third-generation cephalosporin such as cefotaxime. In addition, giving albumin along with the antibiotic reduces kidney injury and death, as a classic trial demonstrated. In people who have already had one episode, or who are at high risk, antibiotic prophylaxis is prescribed to prevent new infections.
Prognosis: why ascites calls for evaluating transplant
The appearance of ascites changes the outlook of cirrhosis. It can be complicated by kidney failure (the hepatorenal syndrome) or by SBP, and both are associated with worse survival. For this reason, the presence of ascites, and especially of refractory ascites or SBP, is considered a signal that a liver transplant evaluation is warranted, since transplant is the only treatment that resolves the underlying liver disease.
None of this means the situation is hopeless. With good salt control, well-adjusted diuretics, timely treatment of infections and a transplant evaluation when appropriate, many people live for years with good quality of life. The key is close follow-up with your hepatology team.
See also
References
- Biggins SW, et al. Diagnosis, Evaluation, and Management of Ascites, Spontaneous Bacterial Peritonitis and Hepatorenal Syndrome: 2021 Practice Guidance by the AASLD. Hepatology. 2021;74(2):1014-1048.
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J Hepatol. 2018;69(2):406-460.
- de Franchis R, et al. Baveno VII - Renewing consensus in portal hypertension. J Hepatol. 2022;76(4):959-974.
- Sort P, et al. Effect of intravenous albumin on renal impairment and mortality in patients with cirrhosis and spontaneous bacterial peritonitis. N Engl J Med. 1999;341(6):403-409.
Related articles
Causes of liver cirrhosis
The causes of cirrhosis, from the most to the least common, and why identifying and treating the cause early can stop and even reverse liver damage.
Hepatology: what it is and what a hepatologist does
Hepatology is the branch of medicine that studies the liver and bile ducts. What a hepatologist does and when you should see one.
Cirrhosis of the liver
Cirrhosis is advanced scarring of the liver. What causes it today, how it is detected, its complications, and why treating the cause can halt or even reverse the damage.