On this page
A liver biopsy is the procedure used to obtain a small sample of the liver so it can be examined under the microscope. With that sample the pathologist can directly see whether there is fat, inflammation or fibrosis (scarring), and often identify the cause of the disease. For decades it was the reference test for knowing what stage a liver disease had reached.
Today the picture has changed: the biopsy is used far less than before. Noninvasive tests, such as elastography (for example FibroScan) and blood indices (such as FIB-4), can estimate the amount of fibrosis without needing to place a needle in the liver. For that reason the biopsy is now reserved for cases where doubt persists or where more than one cause is suspected at the same time.
What is a liver biopsy for?
The biopsy provides information that, in some cases, no other test can give with the same certainty. It comes down to three points:
- Diagnosis. It confirms the suspected condition and, when several possibilities coexist, helps decide which one predominates. It is useful, for example, when autoimmune hepatitis is suspected or when the picture does not fit a single disease.
- Degree of fibrosis (staging). It shows how much scarring the liver has, from normal tissue all the way to cirrhosis. This is the most relevant information, because it defines the prognosis and guides treatment.
- Degree of activity. It shows how much inflammation is present at that moment, which gives an idea of how fast the disease may progress.
Why is it used less than before?
Because most of what we used to seek with a biopsy, above all estimating fibrosis, can now be obtained without a needle. Current liver guidelines recommend starting with noninvasive tests:
- Blood indices, such as FIB-4, which combines age, liver enzymes and platelet count in a simple formula. It is inexpensive and can be calculated from routine tests.
- Elastography, such as FibroScan (transient elastography) or ultrasound-based elastography, which measures the stiffness of the liver: the more fibrosis, the stiffer it is.
These methods are especially reliable at two extremes: to rule out advanced fibrosis in most people and to confirm it when the values are clearly high. They also have obvious advantages: they do not hurt, they require no needle in the liver, they carry no bleeding risk and they can be repeated over time to follow the disease. Because of all this, in conditions as common as fatty liver disease the biopsy is no longer the first step.
The biopsy is therefore left for specific situations: when noninvasive tests give discordant or intermediate results, when more than one disease is suspected at the same time, or when the result will genuinely change the plan (for example, deciding on immunosuppressive treatment in autoimmune hepatitis).
How is it done?
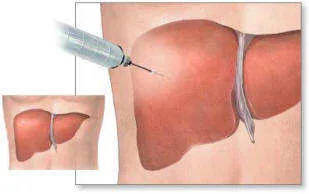
The most common approach is the percutaneous biopsy, that is, through the skin. It can be done as an outpatient or with a short overnight stay. The patient arrives fasting. First the best spot on the right side is located, using percussion or, increasingly, an ultrasound. Then the skin is numbed with local anesthetic and a thin needle is introduced to obtain a small core of tissue. Taking the sample itself lasts less than a second.
There are other routes when the percutaneous approach is not the best option:
- Transjugular biopsy. Through a catheter inserted into the jugular vein in the neck, the liver is reached from inside a vein. It carries a lower bleeding risk, which makes it especially useful in people with clotting problems or with ascites. Its drawback is that the sample tends to be smaller.
- Laparoscopic biopsy or during surgery. It allows the surface of the liver to be seen directly and the puncture site to be controlled more easily. It is used mainly when the person is already going to have an operation for another reason.
- Endoscopic ultrasound-guided biopsy. This is performed during an endoscopic ultrasound, by passing an endoscope through the mouth into the stomach or duodenum. From there, under ultrasound guidance, a fine needle is advanced to obtain a sample of liver tissue.
What are the risks?
A liver biopsy is a routine procedure that, in experienced hands, carries a low risk of complications. Even so, it is not entirely harmless, and that is another reason why noninvasive tests are preferred when they are enough.
The most important complication is bleeding, which occurs in fewer than 1% of cases. It is more frequent in people with clotting problems and in those who have liver tumors. Other, less frequent complications include puncturing a neighboring organ (gallbladder, kidney, lung) and infection. In very exceptional situations one of these complications may require a transfusion or a procedure to resolve it.
To reduce the risk of bleeding, clotting is checked beforehand and it is recommended to stop aspirin and anti-inflammatory drugs during the week before the test, as directed by your physician.
What is the aftercare like?
After the procedure the person rests and is observed for a few hours, usually lying on the right side. It is normal to feel mild to moderate pain on the right side or referred to the right shoulder; it is well controlled with common painkillers.
Once home, it is best to avoid physical exertion and heavy lifting for a few days. You should seek care immediately if you develop severe abdominal pain, dizziness, fainting, fever or difficulty breathing, since these can be signs of a complication.
Do I need a biopsy?
A liver biopsy remains a valuable and very safe tool in expert hands, but it is no longer the first step in evaluating the liver. Today fibrosis is estimated first with blood tests and elastography, and the biopsy is reserved for cases of doubt or when its result will change treatment. If one has been recommended to you, your physician will explain why, in your case, it adds more than what can be obtained without a needle.
See also
References
- Rockey DC, et al. Liver biopsy (AASLD Position Paper). Hepatology. 2009;49(3):1017-1044.
- Sterling RK, et al. AASLD Practice Guideline on imaging-based noninvasive liver disease assessment of hepatic fibrosis and steatosis. Hepatology. 2025;81(2):672-724.
- Patel K, et al. Accuracy of blood-based biomarkers for staging liver fibrosis in chronic liver disease: A systematic review supporting the AASLD Practice Guideline. Hepatology. 2025;81(1):358-379.
- EASL Clinical Practice Guidelines on non-invasive tests for evaluation of liver disease severity and prognosis - 2021 update. J Hepatol. 2021;75(3):659-689.
- Duarte-Rojo A, et al. Imaging-based noninvasive liver disease assessment for staging liver fibrosis in chronic liver disease: A systematic review supporting the AASLD Practice Guideline. Hepatology. 2025;81(2):725-748.
Related articles
Bilirubin: what it is and what a high level means
High bilirubin can be due to hemolysis, Gilbert syndrome, bile duct obstruction or liver disease. How to interpret this test based on its pattern.
Albumin: what a low level means
Albumin is a protein made by the liver. Here is what this blood test measures, why albumin drops in cirrhosis and what other causes it can have.
Prothrombin time and INR
Prothrombin time and INR measure blood clotting and reflect liver function. Why they change in liver disease and what their values mean.