On this page
 Esophageal varices are dilated veins in the wall of the esophagus. They form as a consequence of portal hypertension, the rise in pressure within the portal vein that occurs when the liver is damaged, almost always by cirrhosis. Their main danger is that they can rupture and bleed, which is a medical emergency.
Esophageal varices are dilated veins in the wall of the esophagus. They form as a consequence of portal hypertension, the rise in pressure within the portal vein that occurs when the liver is damaged, almost always by cirrhosis. Their main danger is that they can rupture and bleed, which is a medical emergency.
If you have been told you have esophageal varices, it is important to know that effective treatments exist today both to prevent bleeding and to control it if it happens. Most varices never bleed, and with proper follow-up that risk is reduced even further.
Why do they appear?
When the liver becomes stiff and scarred from cirrhosis, the blood arriving from the intestine and spleen through the portal vein meets resistance as it tries to pass through. That blood looks for alternative routes back to the heart, and one of the main ones runs through the veins of the esophagus and stomach. Subjected to a pressure they are not built for, those veins dilate and form varices.
This rise in pressure is known as portal hypertension. Once it reaches a certain threshold, it is called clinically significant portal hypertension, which is what leads to varices and the risk of complications. The international reference framework for assessing and managing it is the Baveno VII consensus.
Symptoms
Esophageal varices cause no pain or discomfort on their own. The problem arises when they bleed. Variceal bleeding is a serious complication, and its warning signs call for going to an emergency department right away:
- Vomiting blood, either bright red or looking like “coffee grounds” (hematemesis).
- Black, tarry, foul-smelling stools (melena), which indicate digested blood.
- Weakness, dizziness or fainting from blood loss.
- Chronic anemia, when there is small, repeated bleeding, sometimes from portal hypertensive gastropathy.
If any of these signs appear, especially if you have known liver disease, do not wait: go to the emergency room.
Diagnosis
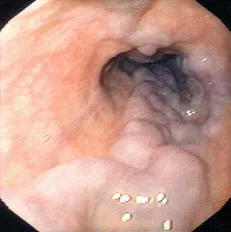
Esophageal or gastric varices are identified with an upper endoscopy, a test that allows the inside of the esophagus and stomach to be seen directly. The size of the varices and certain features on their surface (such as red marks) help estimate the risk that they will bleed.
Not everyone with cirrhosis needs an endoscopy up front. According to Baveno VII, when liver elastography (for example FibroScan) shows low stiffness and the platelet count is within range, the chance of having high-risk varices is very low and endoscopy can be deferred. Your hepatologist will decide what is appropriate in your case.
Preventing the first bleed (primary prophylaxis)
When there has not yet been any bleeding episode, the goal is to prevent the first one. Two strategies of comparable effectiveness are available, and the choice depends on each patient:
- Non-selective beta-blockers. These lower the pressure in the portal vein. Today carvedilol is preferred because it is more potent for this purpose; propranolol and nadolol are also used. Beyond protecting against bleeding, in people with clinically significant portal hypertension these drugs can delay other complications of cirrhosis, such as ascites.
- Endoscopic band ligation. Small rubber bands are placed to strangle the varices until they disappear. It is an option for those who cannot tolerate beta-blockers or have a contraindication.
When the varices are small and low-risk, it is often enough to monitor them and repeat the endoscopy periodically.
Managing acute bleeding
Variceal bleeding is treated in the hospital and combines several measures applied in parallel:
- Stabilization. Blood volume is replaced judiciously, without over-transfusing, and the airway is protected if there is a risk of aspiration.
- Vasoactive drugs. Medications such as terlipressin, somatostatin or octreotide reduce blood flow into the portal territory and help stop the hemorrhage. They are started as soon as the diagnosis is suspected.
- Prophylactic antibiotics. These are given routinely because they reduce infections and improve survival in variceal bleeding.
- Endoscopic ligation. This is the treatment of choice for esophageal varices. For gastric varices, injecting a tissue adhesive (cyanoacrylate) is usually preferred.
When bleeding is not controlled with these measures, or when the risk of it returning is very high, a TIPS (transjugular intrahepatic portosystemic shunt) is used. Through a catheter inserted into a neck vein, a prosthesis (stent) is placed to connect the portal vein with a hepatic vein and decompress the system. In selected high-risk patients, placing the TIPS early improves outcomes. Its main unwanted effect is promoting hepatic encephalopathy.
Preventing further bleeding (secondary prophylaxis)
Once bleeding has occurred, the chance of it recurring is high, so treatment to prevent it is always considered. The current standard combines two measures:
- A non-selective beta-blocker (carvedilol or propranolol), and
- An endoscopic ligation program, with sessions every few weeks until the varices are eradicated, followed by check-ups to make sure they do not return.
In those who bleed again despite this combined treatment, TIPS is the rescue option. This whole process should be managed together with a team experienced in liver disease.
See also
References
- de Franchis R, et al. Baveno VII - Renewing consensus in portal hypertension. J Hepatol. 2022;76(4):959-974.
- Kaplan DE, et al. AASLD Practice Guidance on risk stratification and management of portal hypertension and varices in cirrhosis. Hepatology. 2024;79(5):1180-1211.
- Villanueva C, et al. β blockers to prevent decompensation of cirrhosis in patients with clinically significant portal hypertension (PREDESCI): a randomised, double-blind, placebo-controlled, multicentre trial. Lancet. 2019;393(10181):1597-1608.
Related articles
Causes of liver cirrhosis
The causes of cirrhosis, from the most to the least common, and why identifying and treating the cause early can stop and even reverse liver damage.
Hepatology: what it is and what a hepatologist does
Hepatology is the branch of medicine that studies the liver and bile ducts. What a hepatologist does and when you should see one.
Cirrhosis of the liver
Cirrhosis is advanced scarring of the liver. What causes it today, how it is detected, its complications, and why treating the cause can halt or even reverse the damage.