On this page
Hepatitis D, also called Delta hepatitis, is a liver infection caused by the D virus (HDV). It has one key feature: it can only affect people who already have hepatitis B, because the D virus is defective and needs the B virus in order to multiply. If you do not have hepatitis B, you cannot catch hepatitis D.
It is the most severe form of chronic viral hepatitis. Compared with hepatitis B alone, D virus infection progresses faster to cirrhosis and raises the risk of liver cancer. The good news is twofold: the hepatitis B vaccine also prevents hepatitis D, and there is now a first specific treatment against the D virus.
What is the hepatitis D virus?
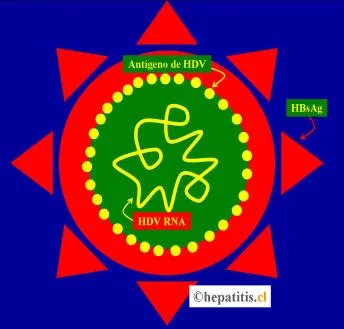
The D virus (HDV, or Delta agent) is a very small, defective virus. Its genetic material is a single circular strand of RNA, wrapped in its own protein (the D antigen, or HDAg). What it cannot make on its own is its outer envelope: for that it uses the hepatitis B surface antigen (HBsAg). This is why the D virus cannot complete its cycle or infect anyone without the B virus being present.
Several genotypes of the virus have been described (1 through 8). Genotype 1 is the most common in the Western world and is associated with a more severe course, while genotype 3, found in the Amazon basin of South America, has been linked to outbreaks of fulminant hepatitis.
How is hepatitis D spread?
The routes of transmission are the same as those of hepatitis B: contact with the blood or body fluids of an infected person. The highest-risk situations are:
- Sharing needles or equipment for injecting drugs.
- Blood contact through non-sterile instruments (tattoos, piercings).
- Unprotected sex.
- Transmission from mother to child, less common than with hepatitis B.
D virus infection can occur in two ways, which carry different prognoses:
- Coinfection: the person catches the B virus and the D virus at the same time. The picture usually resembles acute hepatitis B, though it may be more intense. In most cases both viruses clear together and the infection does not become chronic.
- Superinfection: the person is already a chronic carrier of hepatitis B and then catches the D virus. This is the most dangerous form: it almost always becomes chronic and often accelerates liver damage.
How common is it?
About 5% of people with chronic hepatitis B worldwide are estimated to also have hepatitis D, which amounts to some 12 million people. Prevalence is much higher among those attending liver clinics and in risk groups such as people who inject drugs. The infection is most common in the Mediterranean basin, parts of Africa, Mongolia, Eastern Europe, and regions of the Amazon basin. In Chile it is an uncommon infection.
Does it cause symptoms?
Hepatitis D may cause no symptoms for a long time, like other chronic hepatitis infections. When they appear, they are usually nonspecific: fatigue, general malaise, or discomfort in the right side of the abdomen. In severe acute cases, or when there is already advanced liver damage, there may be jaundice (yellow skin and eyes), dark urine, ascites, or encephalopathy. Because the disease advances faster than other forms of hepatitis, timely diagnosis matters.
How is it diagnosed?
Since the D virus always accompanies the B virus, the first step is a positive HBsAg test. Everyone with hepatitis B is advised to be tested at least once for D virus infection. The workup is done in two stages:
- Anti-HDV antibodies: the screening test. If positive, it indicates contact with the virus.
- HDV RNA: confirms that the virus is active and replicating. This is the test that defines current infection and is used to follow treatment.
In some cases this is complemented by assessing the degree of liver fibrosis with elastography or blood indices, to establish the prognosis.
What is the treatment for hepatitis D?
For decades the only option was pegylated interferon (peginterferon alfa), used for prolonged periods of a year or more. Its effectiveness is limited: only some patients manage to control the virus, and relapses are frequent. The antivirals used for hepatitis B (such as entecavir or tenofovir) do not control the D virus on their own, although they are sometimes continued to treat the underlying hepatitis B.
The most important development is bulevirtide (brand name Hepcludex). It is the first specific drug against the D virus and works as an entry inhibitor: it blocks the receptor the virus uses to enter liver cells. It is given as a daily subcutaneous injection. In the phase 3 MYR301 trial, about half of the patients treated for 48 weeks achieved a virological and biochemical response, far above those who did not receive the drug. More recent studies show that combining bulevirtide with peginterferon improves response rates even further.
Bulevirtide was approved in Europe in 2020 and its use has expanded in several countries. In Chile and much of Latin America, availability is still limited, so treatment decisions should be made with a hepatology team. The optimal duration of treatment is still being defined.
The best strategy is prevention
The most important point for patients is simple: the hepatitis B vaccine also prevents hepatitis D. By blocking B virus infection, the vaccine closes the only entry route for the D virus. Getting vaccinated against hepatitis B, and making sure your children are vaccinated, is the most effective way to avoid Delta hepatitis. For those who already have hepatitis B, avoiding new exposures (not sharing needles, using protection during sex) prevents superinfection.
See also
References
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines on hepatitis delta virus. J Hepatol. 2023;79(2):433-460.
- Wedemeyer H, et al. A Phase 3, Randomized Trial of Bulevirtide in Chronic Hepatitis D. N Engl J Med. 2023;389(1):22-32.
- Asselah T, et al. Bulevirtide Combined with Pegylated Interferon for Chronic Hepatitis D. N Engl J Med. 2024;391(2):133-143.
- Stockdale AJ, et al. The global prevalence of hepatitis D virus infection: Systematic review and meta-analysis. J Hepatol. 2020;73(3):523-532.
Related articles
Types of hepatitis: viral and non-viral
A short guide to the types of hepatitis: viral (A, B, C, D and E) and non-viral (alcohol, fatty liver, autoimmune and toxic), with their differences at a glance.
The 2017 hepatitis A outbreak in Chile
In 2017 Chile had a hepatitis A outbreak with sexual transmission among men. What happened, why more adults are now susceptible, and how the vaccine prevents it.

How to prevent and detect hepatitis
Viral hepatitis can be prevented with vaccines, hygiene and safe practices, and detected with a simple blood test. What to do to protect yourself and who to test.