On this page
Acetaminophen (also called paracetamol) is one of the most widely used painkillers in the world and, taken at the correct dose, it is safe. The problem is overdose: in excess, acetaminophen damages the liver and is today one of the leading causes of acute liver failure in many countries. If you or someone close to you has taken more acetaminophen than they should, the right response is to go to an emergency department right away, even with no symptoms at all.
The reason for that urgency is simple: there is an antidote, N-acetylcysteine, that is highly effective when given in time, especially within the first few hours. The earlier treatment starts, the lower the risk of serious damage. That is why the outcome depends, more than on anything else, on recognizing the problem early and acting fast.
What is the toxic dose?
In an adult, the maximum recommended dose is 4 grams per day (for example, eight 500 mg tablets). In children it is calculated by body weight, up to a maximum of 80 mg/kg per day.
The risk of liver damage appears above those figures:
- In adults, a single intake greater than about 10 grams or 150 mg/kg is considered potentially toxic.
- In children, the threshold is also around 150 mg/kg.
These numbers are a guide, not exact lines. Some people are harmed by lower doses because their liver has fewer defenses against acetaminophen. It is worth knowing the factors that raise the risk:
- Fasting and malnutrition. They lower reserves of glutathione, the substance the liver uses to neutralize the toxic metabolite.
- Chronic alcohol use. It ramps up the enzymes that produce that metabolite and often goes with poor nutrition.
- Medications that induce those same liver enzymes (some anticonvulsants and antituberculosis drugs, among others).
- Pre-existing liver disease or genetic factors, such as a reduced ability to clear the drug (for example, in Gilbert syndrome).
An important point for everyday life: many poisonings are not intentional but happen by unknowingly adding up several products that contain acetaminophen (cold remedies, combination painkillers, cough syrups). It is easy to exceed 4 grams a day when the same compound is in three different medicines.
How does acetaminophen damage the liver?
At normal doses, the liver turns almost all of the acetaminophen into harmless compounds that leave the body in the urine. Only a small fraction goes through a different pathway that produces a highly reactive metabolite called NAPQI (N-acetyl-p-benzoquinone imine). The liver neutralizes that NAPQI immediately thanks to glutathione, a natural antioxidant.
When the dose is high, the safe pathways become saturated and far more NAPQI is made. At the same time, glutathione reserves run out. With no glutathione to neutralize it, NAPQI binds to liver cells and destroys them. This is why fasting and chronic alcohol use, which lower glutathione, make the same dose more dangerous. And it is why the antidote works: N-acetylcysteine replenishes glutathione and helps inactivate NAPQI before it causes harm.
What symptoms does it cause?
A key and deceptive fact: in the early hours the person may feel perfectly well or have only mild nausea and malaise. Those early symptoms do not reflect the severity of what is to come. The typical course unfolds in stages:
- First 24 hours: nausea, vomiting or fatigue, or no symptoms at all.
- 24 to 72 hours: pain appears in the right side of the abdomen and the liver blood tests begin to change.
- 72 to 96 hours: this is when damage peaks. Liver enzymes can be extremely high, and there may be jaundice (yellowing of skin and eyes), clotting problems and encephalopathy (confusion from liver failure). The kidneys are often affected as well.
- 4 days to 2 weeks: those who get through the critical phase recover gradually. Acetaminophen leaves no chronic liver damage; a liver that survives regenerates completely.
Precisely because the early symptoms are so unremarkable, there is no room to “wait and see.” The decision to seek care is based on how much was taken, not on how the person feels.
How is it diagnosed?
In the emergency department, the first step is to estimate how much acetaminophen was taken and when. If the intake was a suicide attempt, other substances are looked for as well.
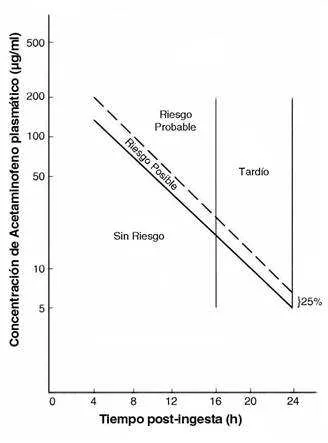
The central tool is measuring the blood acetaminophen level. It must be drawn between 4 and 24 hours after the intake: before 4 hours the value is not reliable for making decisions. The result is interpreted with the Rumack-Matthew nomogram, a chart that plots the blood level against hours elapsed and defines whether there is a risk of liver damage and, therefore, whether the antidote should be started.
Diagnosis is harder when the excess intake was chronic or repeated, because symptoms are more subtle and the history of the dose is not always available. It should be suspected in anyone with risk factors (alcohol use, fasting, use of enzyme inducers) who has taken more than 4 grams a day and shows abnormal liver tests.
Treatment: N-acetylcysteine as the antidote
Treatment rests on two measures.
- Decontamination with activated charcoal. Used for people who arrive within the first few hours of ingestion. The charcoal traps acetaminophen in the gut and reduces how much is absorbed.
- N-acetylcysteine (NAC). This is the antidote. It replenishes glutathione, helps neutralize NAPQI and, in later phases, provides antioxidant and anti-inflammatory effects.
The decisive factor is time. N-acetylcysteine is most effective when started within the first 8 to 10 hours after ingestion; within that window it prevents liver damage in the large majority of cases. Given late it still offers benefit, so it is used even when more time has passed, but the margin narrows. This is the best reason not to delay seeking care.
N-acetylcysteine is indicated, among other situations, when:
- The acetaminophen level falls above the risk line on the nomogram.
- The intake was clearly high and the level cannot be measured in time.
- There is evidence of liver damage on the tests.
In Chile the available form is oral. The intravenous formulation, standard in Europe, is not always available. N-acetylcysteine has an unpleasant taste and smell and can cause nausea, which eases when it is mixed with juice or a cold drink and antiemetics are used. In very large overdoses the antidote dose may need to be increased.
When is a transplant needed?
Most patients treated in time recover with no lasting effects. In a minority, however, damage progresses to fulminant liver failure, and then a liver transplant can be the only chance of survival.
To decide who needs a transplant, the King’s College criteria are used, developed specifically for acetaminophen poisoning. They point to a poor prognosis without transplant when there is:
- Arterial pH below 7.3, or
- The combination of advanced encephalopathy (grade III or IV), a severe clotting disturbance (markedly prolonged prothrombin time) and kidney failure (elevated creatinine).
A high lactate that does not improve after fluid resuscitation also signals a poor prognosis. Any patient progressing to severe liver failure should be assessed early by a transplant team.
How to prevent poisoning
Prevention is simple and effective:
- Respect the maximum dose of 4 grams a day in adults (less if there is liver disease, alcohol use or malnutrition), and calculate by weight in children.
- Read the labels. Do not combine several acetaminophen-containing products at the same time (cold remedies, painkillers and syrups often contain it).
- Be especially careful if you drink alcohol regularly or are fasting for a long time.
- Keep medicines out of the reach of children.
If you have any doubt about a possible overdose, contact your local poison information center or go directly to an emergency department. In acetaminophen poisoning, seeking care early makes all the difference.
See also
References
- Chidiac AS, et al. Paracetamol (acetaminophen) overdose and hepatotoxicity: mechanism, treatment, prevention measures, and estimates of burden of disease. Expert Opin Drug Metab Toxicol. 2023;19(5):297-317.
- Licata A, et al. N-Acetylcysteine for Preventing Acetaminophen-Induced Liver Injury: A Comprehensive Review. Front Pharmacol. 2022;13:828565.
- Akakpo JY, et al. Comparing N-acetylcysteine and 4-methylpyrazole as antidotes for acetaminophen overdose. Arch Toxicol. 2022;96(2):453-465.
- Hendrickson RG. What is the most appropriate dose of N-acetylcysteine after massive acetaminophen overdose? Clin Toxicol (Phila). 2019;57(8):686-691.
- Polson J, Lee WM. AASLD position paper: the management of acute liver failure. Hepatology. 2005;41(5):1179-1197.
Related articles
Hepatotoxic mushroom poisoning (Amanita phalloides)
Eating wild Amanita mushrooms can cause acute liver failure from amatoxins. Clinical phases, treatment and why it is a medical emergency.
The myth of the daily glass of wine: is moderate drinking good for you?
A daily glass of wine is not a healthy habit. Current evidence shows there is no risk-free level of alcohol, either for the heart or for the liver.
Bilirubin: what it is and what a high level means
High bilirubin can be due to hemolysis, Gilbert syndrome, bile duct obstruction or liver disease. How to interpret this test based on its pattern.