On this page
Focal nodular hyperplasia (FNH) is a benign liver tumor, the second most common after the hemangioma. If you were found to have an FNH on an ultrasound or a CT scan, the most important message is reassuring: it is a benign lesion that does not turn into cancer and that, in the vast majority of cases, causes no symptoms and needs no treatment.
FNH can appear at any age and in both sexes, but it is clearly more common in young women, between the ages of 20 and 50. It is almost always discovered by chance, on imaging ordered for another reason or during a routine check-up. The key to its management is reaching the correct diagnosis and avoiding unnecessary tests or surgery.
What is it and why does it happen?
Focal nodular hyperplasia is not a “true” tumor in the sense of uncontrolled cell growth. It is considered a response of normal liver tissue to an abnormal artery, larger than expected, usually located at the center of the lesion. That artery delivers increased blood flow, and the liver reacts by forming a nodule of nearly normal tissue around it.
That is why FNH contains hepatocytes (the liver’s own cells), Kupffer cells and small bile ducts, all arranged around a central scar of connective tissue. This central scar is the feature that distinguishes it and that greatly helps in diagnosis. There is a variant called telangiectatic, now reclassified as a type of adenoma, which tends to be multifocal and lacks the typical central scar.
Unlike the hepatic adenoma, FNH has no clear link to contraceptives and carries no risk of turning into cancer.
Does it cause symptoms?
Usually not. The vast majority of people with FNH have no symptoms at all, and the lesion is found incidentally on tests done for other reasons. When there is discomfort, it is nonspecific: mild pain in the right side, a sense of a mass or early fullness, almost always with large nodules. Complications such as bleeding or infarction of the lesion are truly exceptional, unlike what happens with an adenoma.
How is it diagnosed?
The diagnosis of FNH rests mainly on imaging studies. Only in exceptional cases is a biopsy or resection needed to confirm it. The most useful studies are:
- Abdominal ultrasound. Usually the first test. FNH may appear as a lesion of variable size, lighter or darker than the surrounding liver. Doppler study can show the arterial blood-flow pattern, with vessels running from the center outward (a “spoke-wheel” pattern).
- MRI with a liver-specific (hepatocyte) contrast agent. This is now the preferred test. When it shows the typical features, including uptake of contrast by the central scar on delayed phases, it reaches very high specificity and usually suffices to confirm the diagnosis without a biopsy.
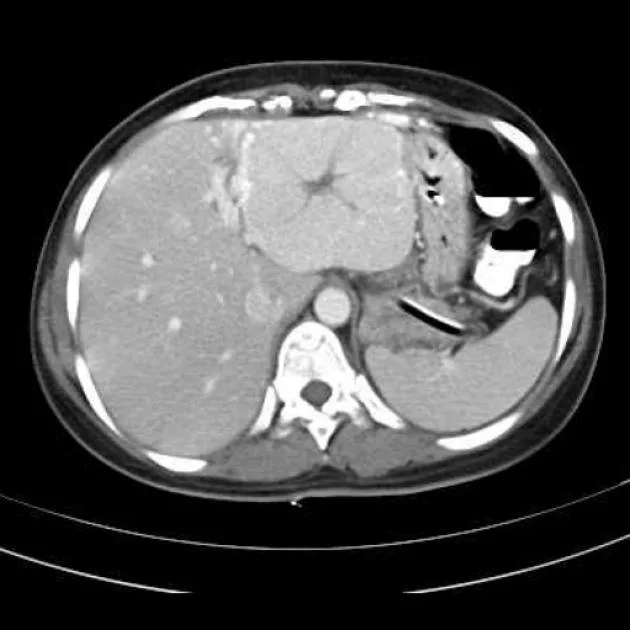
- Triple-phase CT scan. It also provides a great deal of information: it shows a nodule that enhances intensely in the arterial phase and a characteristic central scar.
- Blood tests. Liver tests (liver enzymes and liver function tests) and alpha-fetoprotein are usually normal. Screening for hepatitis B and hepatitis C is often requested as part of the work-up of any liver lesion.
When the imaging is typical, nothing else is needed. Biopsy is reserved for cases where doubt persists between FNH and other lesions.
How is it different from a hepatic adenoma?
This is the most important distinction, because it completely changes the prognosis and the management. Although both are benign tumors and more common in women, their risks differ:
- Focal nodular hyperplasia: does not become cancer, almost never bleeds and has no clear link to oral contraceptives. In general it is enough to confirm it and watch it.
- Hepatic adenoma: can bleed and, in certain subtypes and sizes, carries a small risk of turning into liver cancer. It is associated with long-term use of oral contraceptives and with anabolic steroids, and it often requires stopping those hormones, close follow-up or surgery when large.
Other conditions the physician considers include liver hemangioma, hepatocellular carcinoma and metastases. That is why the key point of the evaluation is the correct diagnosis.
Does it need treatment? Should I stop contraceptives?
In the vast majority of cases, no. Because FNH is benign, does not become cancer and is almost always symptom-free, the usual approach is no treatment at all. The size of the lesion tends to stay stable over time, and it may even shrink.
Regarding contraceptives, current guidelines are clear: unlike an adenoma, there is no need to stop oral contraceptives simply because of an FNH, nor do they contraindicate a pregnancy. There may be exceptions for large lesions or when the diagnosis is uncertain, something your physician will assess case by case.
Usual follow-up consists of repeating an imaging study (typically an ultrasound or MRI) after some time to confirm that the lesion remains stable. If it does, many specialists stop the checks. Surgery is reserved for very uncommon situations: lesions that clearly grow, that cause persistent symptoms, or when an adenoma or another tumor cannot be safely ruled out.
The bottom line
Focal nodular hyperplasia is a common and, above all, benign finding. It does not turn into cancer, rarely causes problems and, when MRI shows its typical features, there is no need to biopsy or operate on the liver. The most important thing is to tell it apart from an adenoma and reach a confident diagnosis, so the person can be reassured and unnecessary procedures avoided.
See also
References
- European Association for the Study of the Liver (EASL). EASL Clinical Practice Guidelines on the management of benign liver tumours. J Hepatol. 2016;65(2):386-398.
- Frenette C, et al. ACG Clinical Guideline: Focal Liver Lesions. Am J Gastroenterol. 2024;119(7):1235-1271.
- Myers L, Ahn J. Focal Nodular Hyperplasia and Hepatic Adenoma: Evaluation and Management. Clin Liver Dis. 2020;24(3):389-403.
- Reguram R, et al. Practical approach to diagnose and manage benign liver masses. Hepatol Commun. 2024;8(11):e0560.
Related articles

Liver hemangioma
A liver hemangioma is the most common benign liver tumor. It is almost always an incidental finding, causes no symptoms and needs no treatment.
Polycystic liver disease
Polycystic liver disease means multiple cysts in the liver of genetic origin. It is usually symptom-free and liver function is preserved. What it is and when it is treated.
Simple liver cyst
A simple liver cyst is a fluid-filled cavity, very common and benign. It is almost always an incidental finding that causes no symptoms and needs no treatment.