On this page
If you arrived here searching for “treating hepatitis C with ezetimibe,” let us be clear from the start: ezetimibe is not a treatment for hepatitis C. Hepatitis C is cured today with direct-acting antivirals, which clear the virus in more than 95% of cases. What follows is the story of a line of research, not a treatment recommendation.
This page describes a research project we carried out some years ago, when the treatment landscape was still changing quickly. The idea was to explore whether a cheap, already available cholesterol drug, ezetimibe, could add something against the virus. It is a piece of science communication and history. We keep it because it shows how a hypothesis is tested, but ezetimibe remained a laboratory finding, not a clinical therapy.
The hypothesis: blocking the virus’s entry door
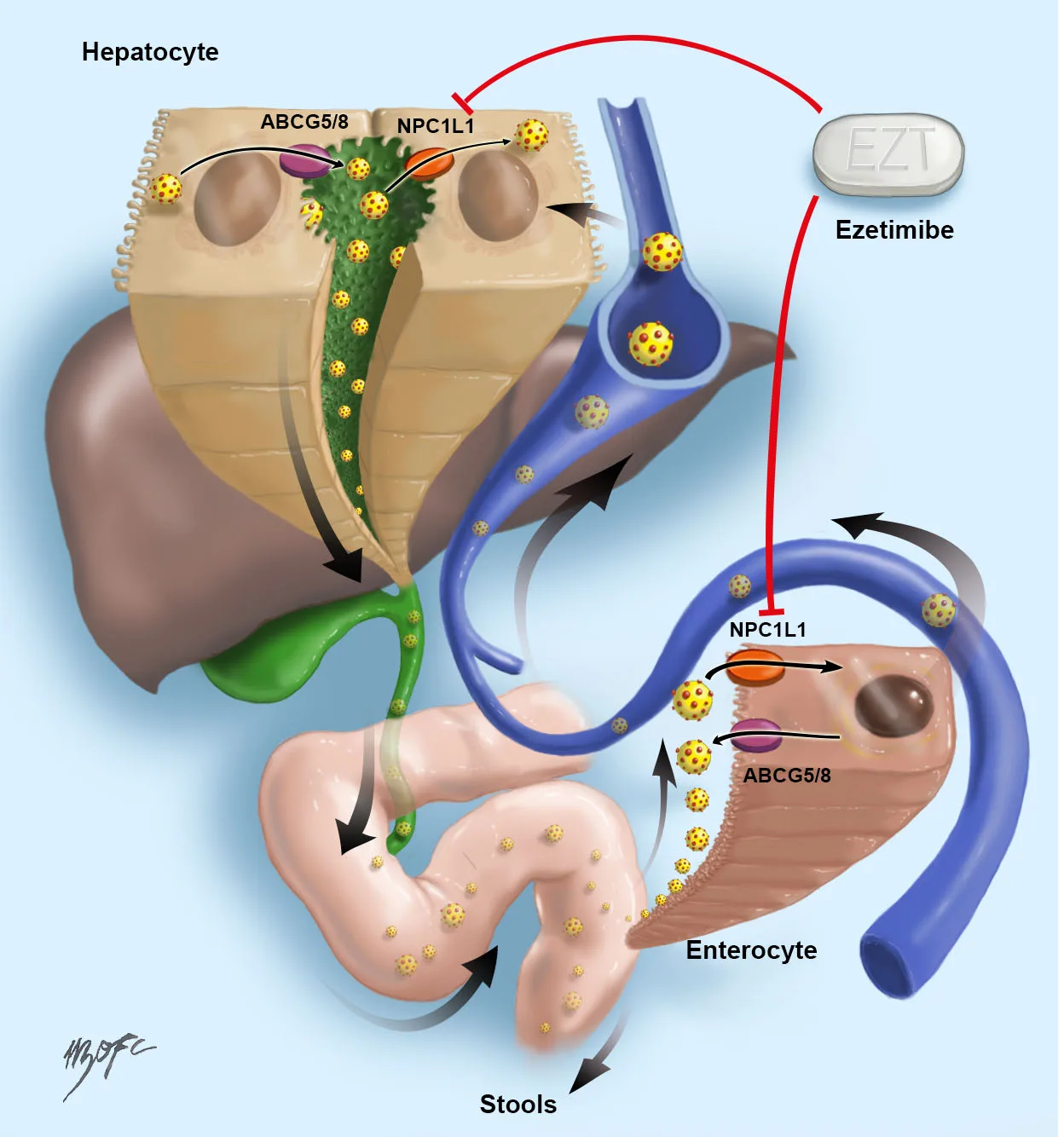
To infect a liver cell, the hepatitis C virus needs to use several “doors” on the surface of the hepatocyte. In 2012 a group described that one of those doors is NPC1L1 (Niemann-Pick C1-like 1), a cholesterol-transport protein found in the intestine and in the membrane of liver cells. That same transporter is the target of ezetimibe, a drug approved years ago to lower cholesterol.
An appealing idea followed from this. If ezetimibe blocks NPC1L1, it might get in the way of the virus entering the cell. In laboratory experiments (in vitro and in animal models) ezetimibe delayed infection of cells by the C virus. Our group also proposed that the virus might have an “entero-hepatic” cycle similar to that of cholesterol, which could likewise be interrupted with this drug.
What we studied in patients
The goal was to put that hypothesis to the test in people with hepatitis C, in two different settings:
- Stable chronic infection: ezetimibe was given at a dose of 20 mg a day for 12 weeks. Viral load (the virus’s RNA) was measured in plasma, bile and stool, before, during and after treatment.
- Patients on the liver transplant list: ezetimibe 10 mg a day was used to see whether the drug could curb reinfection of the new liver, a classic problem in transplantation for hepatitis C.
We also wanted to know whether certain genetic variants of the NPC1L1 protein influenced the response.
What we found
The results were modest and honest:
- In chronic infection there was a very slight drop in viral load in plasma, but not in bile or stool, and in no case did the virus become undetectable.
- In transplant patients ezetimibe was well tolerated and lowered the viral load in plasma somewhat, but it did not prevent reinfection of the graft: within a few weeks patients returned to their baseline viral load.
- The genetic variants of NPC1L1 did not explain the differences between patients.
The practical conclusion is simple. As a single agent, ezetimibe does not treat or eradicate hepatitis C. At the time we suggested it might have an additive effect alongside antivirals, much as the old ribavirin helped interferon. That idea never reached clinical practice, and with the arrival of direct-acting antivirals it was no longer needed.
How hepatitis C is treated today
This is the point that matters most for a patient. Hepatitis C is treated today with direct-acting antivirals (DAAs), tablets taken for 8 to 12 weeks, with very few side effects and cure rates (sustained virologic response) above 95%. The most widely used regimens are pangenotypic, meaning they work for nearly all genotypes of the virus:
- Sofosbuvir/velpatasvir.
- Glecaprevir/pibrentasvir.
Current guidelines (AASLD-IDSA in the United States and EASL in Europe) recommend treating almost everyone with chronic infection, and in Chile hepatitis C treatment is covered by guaranteed benefits. Ezetimibe is not part of any of these regimens. It remains what it always was: a cholesterol medication.
What to keep in mind
If you have been diagnosed with hepatitis C, the path is not ezetimibe but seeking care to receive direct-acting antivirals, which cure the infection in the vast majority of cases. The ezetimibe work described here was laboratory and early clinical research: it added knowledge about how the virus enters the cell, but it did not change treatment.
See also
References
- Sainz B, et al. Identification of the Niemann-Pick C1-like 1 cholesterol absorption receptor as a new hepatitis C virus entry factor. Nat Med. 2012;18(2):281-285.
- Del Campo JA, Rojas Á, Romero-Gómez M. Entry of hepatitis C virus into the cell: a therapeutic target. World J Gastroenterol. 2012;18(33):4481-4485.
- Monrroy H, López-Lastra M, Soza A. Hepatitis C virus may have an entero-hepatic cycle which could be blocked with ezetimibe. Med Hypotheses. 2017;102:51-55.
- Ghany MG, et al (AASLD-IDSA). Hepatitis C Guidance 2023 Update: AASLD-IDSA Recommendations for Testing, Managing, and Treating Hepatitis C Virus Infection. Clin Infect Dis. 2023.
- European Association for the Study of the Liver. EASL recommendations on treatment of hepatitis C: Final update of the series. J Hepatol. 2020;73(5):1170-1218.
Related articles
Bilirubin: what it is and what a high level means
High bilirubin can be due to hemolysis, Gilbert syndrome, bile duct obstruction or liver disease. How to interpret this test based on its pattern.

Liver transplant
A liver transplant replaces a diseased liver with a healthy one. Who is a candidate, how patients are prioritized with the MELD score, and what to expect from the process.
Types of hepatitis: viral and non-viral
A short guide to the types of hepatitis: viral (A, B, C, D and E) and non-viral (alcohol, fatty liver, autoimmune and toxic), with their differences at a glance.